Human Vision Response in AR & VR 2016.12.19
Ying-Shan Chen, Yi-Pai Huang* , Chien-Yu Chen**
Cathay General Hospital , Taiwan
*National Chiao-Tung University , Taiwan
**National Taiwan University of Science and Technology , Taiwan
Keywords: vision response; visual discomfort; AR/VR display
ABSTRACT
AR & VR display technology had been developed and expanded rapidly in recent years. Human factors in 3D depth perception right then becomes a very important issue. Because the human vision response in AR &VR is definitely different from stereoptic images created by human macula of the real world.Macula is in the center of retina which create most important vision for human brain to recognize the images. During the general eye usage, macula in not so important for wide field image. However, macula will receive heavy light dosage when playing AR & VR. Therefore, under the responded command of macula, ciliary muscle contraction will help to precise focusing on macula. Under using AR &VR for a long period, macula will over receive the blue light emissive by the display of AR/VR, and also the ciliary muscle spasm will cause eye strain and pseudomyopia. However, the pupil constriction during near vision will lower the eye pressure, thus can help release the eye fatigue when watching AR & VR. According to the previous vision analysis, the index of physiological measurement for visual response should be developed and standardized in order to improve the AR & VR display in the future.
OBJECTIVE AND BACKGROUND
Emerging AR & VR displays may cause visual discomfort and poor playing experience. There are many potential sources when playing AR/VR that could arouse discomfort [1]. Physiological issues are probably among the most common reason to be discussed. And the visual presentation of sickness is extremely important[2]. Due to majority of information input from sensory organs to the brain is from vision [3]. The collection, processing and interpretation of visual data in the brain is the goal importance for AR/VR to work. Macula is in the center of retina. Its area is only 5% of retina, but its electrical visual impulse through optic nerve to the brain using 50% of the brain volume to form the most central 20∘ field. When discussing the visual response in AR/VR devices, macula will take the full responsibility to receive the display screen image information (Fig.1) [6].
Macula is the stereopsis engine that when combine both eyes together they could make up the vivid 3D image [7]. Macula take full charge of the near vision follow the order of visual brain [8]. For receiving clear focus of macula, 3 sets of muscles needed to function together. The major muscles include ciliary muscle, pupil muscle and extra-ocular muscles (Fig.2) [9]. The first 2 pairs make monocular image clear and last group of muscles ensure binocular one image. IF all muscle pairs work precisely, through clearly in focus of both eyes. 3D image could be created in the visual brain [10]. Macula is expert in creating stereopic image formation under the command of the visual brain, and also have great optical tolerances in near work.
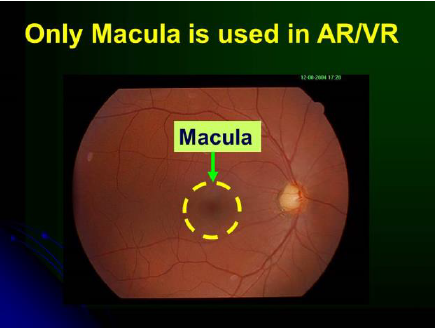
Fig. 1 Only Macula is used in AR/VR
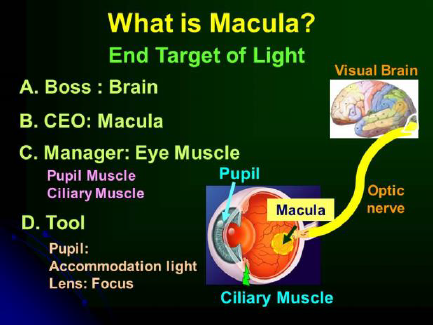
Fig. 2 What is Macula?
The health issues associated with VR usage concerning visual damage all come from light [11]. Eyes generally feel unpleasant using AR/VR equipments may come from overload receving of the incoming light. In
monocular point of view, it will cause ciliary spasm or paralyisis due to focusing problem [12]. Asthenopia and visual fatigue is its major side effects (Fig.3).
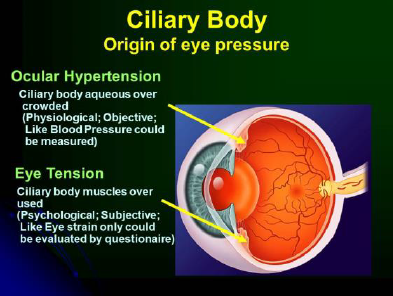
Fig. 3 Ciliary body
And blue light accumulative effect to lens and retina will cause more serious complications. Long term of heavy light dependent AR/VR work will induce chronic inflammatory reaction (Fig.4), finally lens opacity and macular edema will formed [13]. Discussing binocular viewing, mismatch between accommodation and convergence is most frequently considered (Fig.5).
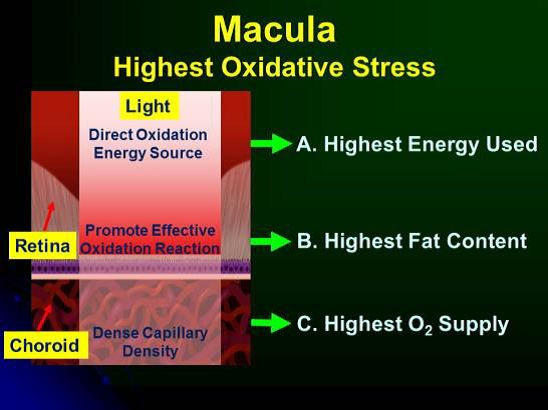
Fig. 4 Macula: Highest Oxidative Stress
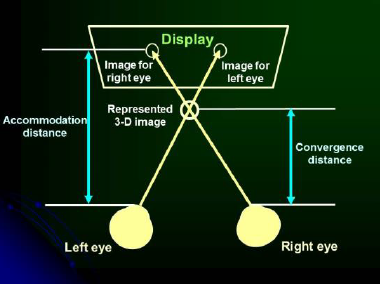
Fig. 5 Mismatch between accommodation and convergence
Transient binocular visual acuity reduction, nausea, headache are major complaints from the users [14]. The reason why stereoptic displays will cause visual stress is due to constant accommodative demand but changing geometric depths in virtual world to have different convergence demand (Fig.6) [15]. Simulator sickness symptom is currently regarded as the most popular discomforts in AR/VR users [16]. It is due to sensory conflict occurs when signals from the various sensory organs that are in conflict with one another. When brain receiving signals that are different from past experience motion sickness aroused (Fig.7) [17] [18].
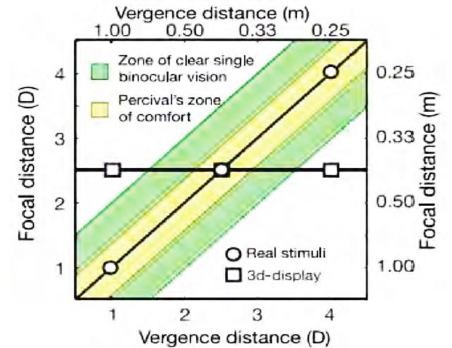
Fig. 6 Visual stress is due to constant accommodative demand but changing geometric depths in virtual world to have different convergence demand
The index of physiological measurement is important in AR/VR future evolving. The main goal of this presentation is to give the researchers, especially the non-medical teams some useful concepts how the eyes will form 3D images and discuss the possible AR/VR discomfort factors will affect the eyes and body. And also some assessment methods in order that they could have proper thinking references of human factors engineering in developing 3D monitors in the future.
PHYSIOLOGICAL ASSESSMENT
There are many different methods to assess the fatigue induced by viewing AR/VR displays.
A. Systemic physiological measurement
There are many items concerning physiological response that could indicate user’s systemic feedback after AR/VR usage. When sympathetic reaction is stronger, it will induce heart rate increase, respiratory rate increase, skin thermal temperature increase and also Galvanic skin response (GSR), will also increase. These vital signs of the body are good indications of stressful tension condition. Fatigue and anxiety will soon be apparent afterward (Table 1).
B. Eye Local Change:
a. Visual acuity and Refractive error
Long term near work, will induce visual fatigue and increase pseudomyopia. Using E-chart and refractometry will be the basic assessment tools.
b. Accommodation Sensitivity
Indicate the time needed from detecting the visual stimulation to complete focusing. In the period of eye fatigue and discomfort the accommodation sensitivity decrease is noted.
c. Pupil size
There is a conflict between near vision and sympathetic tone. Because in near vison the pupil constriction but when in excitation mood the sympathetic tone dominant that pupil tende to be dilated.
d. Intraocular Pressure
Indicate the actural measurable pressure of the eyeball. Higher the pressure, easier the optic nerve damage and worse visual field defect (Fig.8).
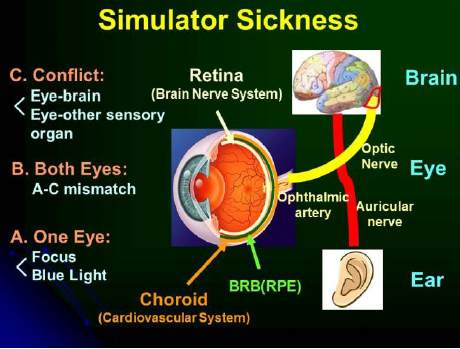
Fig. 7 Simulator Sickness
Table 1 Levels of Simulator Sickness
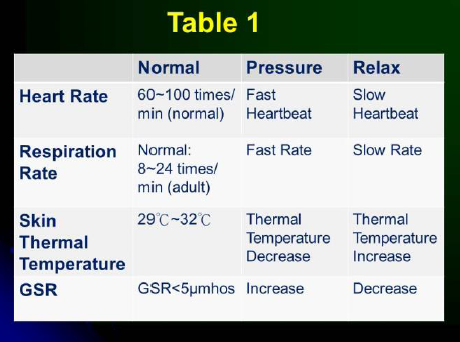
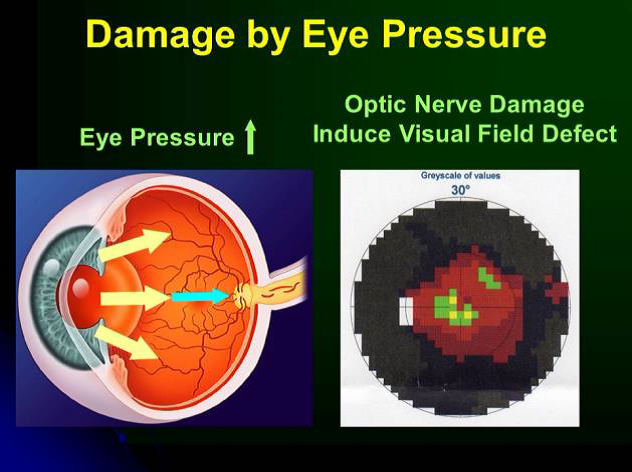
Fig. 8 Damage of Eye Pressure
C. Special Ocular Examination
a. Contrast Sensitivity Function (CSF)
Discremination ability of the eye toward a frequency and object brightness difference.
b. Critical Fusion Frequency (CFF)
Ability to tell the difference of two consecutive stimuli. Photoreceptors decrease this ability in case of fatigue and discomfort.
c. Microperimetry(μVF): Detect retinal light sensitivity central 6∘,or 10∘ of macula area. Precise detect macula function.
d. Ciliary muscle functional test: For evaluating ciliary muscle function, and also its contracture state will also be assessed (Fig.9).
Fig.
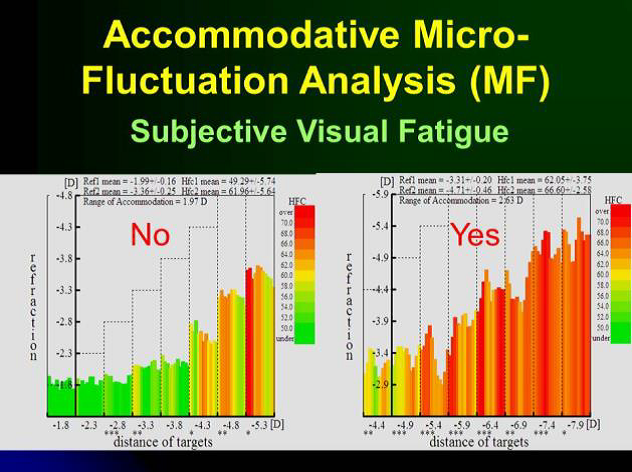
Fig. 9 Ciliary Muscle Function Test
CONCLUSION
Study into the side effects of AR/VR use is difficult and complex. No only because VR techniques are quite new but also macula and brain are the spiritual organ and tissue that are hard to evaluate [19]. Macula is the window of brain, Macula control many sets of muscles to
work on sharp in focus image, and for brain to create stereopsis image. Conflict between macula and brain produce a big impact in the genesis of symptoms. Evaluate the visual response during AR/VR and assess the visual threshold is important for present user to avoid potential discomforts [20]. Presently, human factors research has improved and reduces some proposed causative factors.
Considering risk of increase eye tension, those of Glaucoma patient, Cataract with poor contrast sensitivity (Fig.10) [21], and presbyopia with poor accommodation power, and heavy light dependent workers of high myopes, should reduce the AR/VR displays time or have break intervals to ensure eyes have some rest to avoid long term possible damage [22] [23].
Fig.
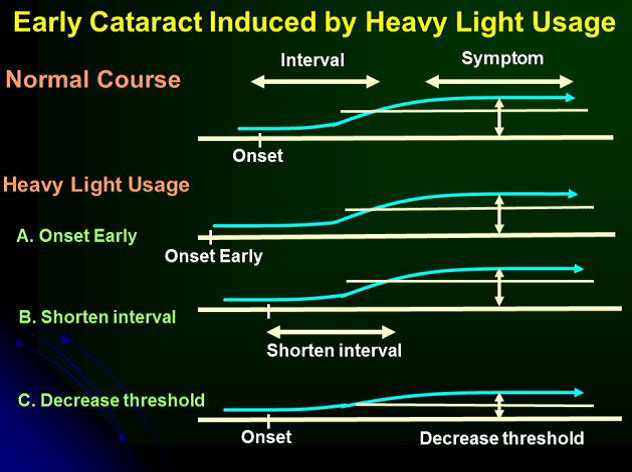
Fig. 10 Early Cataract Induced by Heavy Light Usage
REFERENCES
[1] American Journal of Optometry and Physiological Optics, 65(3):162-167.
[2] Gupta, S.C., Wantland, C.A. and Klein, S.A. (1996). Cyberpathology: Medical Concerns of VR Applications. Journal of Medicine and Virtual Reality, 1996, 1(2):8-11.
[3] Howarth, P.A. (1996) Empirical Studies of Accommodation, Convergence, and HMD Use. Proceedings of the Hoso-Bunka Foundation Symposium, Tokyo, December 3 1996.
[4] Chen Ying-Shan, “Double macula make up 3D image-Formation of steoptic image and howit induce tension,” Cathay Medical Center Medical News Letters, 2010, 127: 20-22
[5] Chen Ying-Shan, “Age-Related Macular degeneration-Killer of the vision of senile people,” Health World Publication, 2006, Chap2.
[6] Chen Ying-Shan, “From iPad to Eyetension, Cathay Medical Center Medical News Letters, “ 2010, 123:12-14.
[7] Mon-Williams, M. and Pascal, E.(1995). Virtual Reality Displays, Implications for Optomerrists. Optometry Today, Jan. 30th, PP 30-33.
[8] Kennedy, R.S. and Frank, L.H, “A review of motion sickness with special reference to simulator
sickness. (AD-A155 975), p.45. Canyon Research Group, Inc., Westlake Village, CA, 1985, 15th Apr.
[9] McCauley, M.E. and Sharkey, T.J., “Cybersickness: Perception of Self-Motion in Virtual Environments,” 1991, Presence, 1, pp 311-317.
[10] National Research Council. (1983). Visual Display, Work and Vision. National Academy Press.
[11] Pausch, R., Crea, T. and Conway, M., “A Literature Survey for Virtual Environments: Military Flight Simulator Visual Systems and Simulator Sickness,” 1992, Presence, Vol. 1, No. 3, pp 344-363.
[12] J. Parker, “Binocular depth perception and the cerebral cortex,” Nat. Rev. Neurosci, 2007, 8: 379–391.
[13] Marc Lambooij and Wijnand IJsselsteijn, “Visual Discomfort and Visual Fatigue of Stereoscopic Displays: A Review,” Journal of Imaging Science and Technology, 2009, 53(3):030201-030201-14.
[14] D.L. Ehrlich, “Near vision stress: vergence adaptation and accommodative fatigue Ophthalmic and Physiological Optics,” 1987, 7 (4): 353–357.
[15] Shibata, T., Kawai, T., Ohta, K., Otsuki, M.,Miyake, N., Yoshihara, Y., and Iwasaki, T., “Stereoscopic 3-D display with optical correction for the reduction of the discrepancy between accommodation and convergence,” Journal of SID, 2005, 13(8): 665-671.
[16] Hoffman,D., Girshick,A. , Akeley,K., and Banks,M., “Vergence-accommodation conflicts hinder visual performance and cause visual fatigue,” Journal of Vision, 2008, 8(3):33, 1–30
[17] Ying-Ying Ko, Chien-Wen Chen,Ren-Lang Dong, & Ying-Shan Chen, “The cause offatigue that induced by viewing 3D image and its physiological measurement,” Optical Engineering, 2011, 116: 49-54
[18] Tyler CW, Scott AB: Binocular vision, in Records RE, ed: Physiology of the human eye and visual system, Hagerstown, MD: Harper & Row, 1979, pp643-671.
[19] G. Cumming and G. C. DeAngelis, “The Physiology of Stereopsis”, Annu. Rev. Neurosci, 2001, 24:203-238.
[20] Fatigue in Visual Display Terminal (VDT) Work. Acta Ophthalmologica, Supplement 185: 175-176.
[21] Shotton, M.A. (1989). Computer Addication? A Study of Computer Dependancy. Taylor and Francis.
[22] Viirre, E.(1994). A Survey of Medical Issues and Virtual Reality Technology. Virtual Reality World, August, pp 16-24.
[23] Wilson, J.R.(1996). Effects of participating in virtual environments: A review of current knowledge. Safety Science, Vol. 23, No.1, pp 39-51.
3C護眼達人陳瑩山 黃斑部病變 乾眼症 飛蚊症 眼中風 白內障 老花眼 高度近視 糖尿病眼底病變 青光眼 夜盲症 3C眼
